What is pulmonary embolism (PE)?
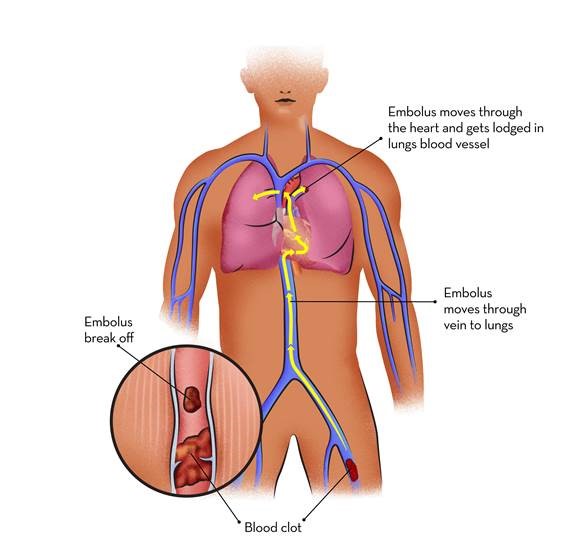
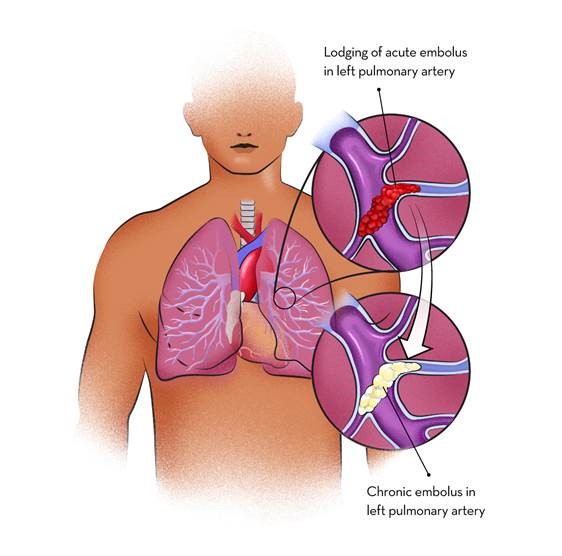
Acute saddle pulmonary embolism is a condition in which a large pulmonary embolism at the pulmonary trunk straddles both right and left pulmonary artery branches. If untreated, it can be fatal.
What are the causes of pulmonary embolism?
How is a pulmonary embolism diagnosed?
What is pulmonary thrombo endarterectomy (PTE) surgery?
Pulmonary thromboendarterectomy (PTE) is one of the most difficult operations to master in cardiothoracic surgery. This procedure requires a long learning curve and consequently, there are less than 50 surgeons in the world who have had an experience of performing more than 500 operations, the outcomes improve with more experience. Post-operative management in patients who have had PTE is not the same as treating other post-operative cardiac surgical patients and requires intense monitoring, specialized training and experience. Many of the complications of this operation require the patient to be treated with ECMO, though most people can put a patient on ECMO, managing these patients require a lot of experience. At Narayana Health we have a cumulative experience of nearly 1,000 ECMO runs. A multidisciplinary team is involved in the evaluation of each and every patient to decide on the best way of treatment, which is known to improve the outcomes. The unpredictability of financial burden to the patient in case of complications or need for ECMO (which can far exceed the original estimate of operation cost) is offered as part of the operative package assuring predictability of expenses related to the operation. An expert centre for this disease, by definition, needs to have a volume of over 50 operations annually and be able to offer all the therapeutic options for these patients.
At present, no other hospital in the subcontinent meets the volume criteria for being an expert centre.
Pulmonary thromboendarterectomy (PTE) is one of the most difficult operations to master in cardiothoracic surgery. This procedure requires a long learning curve and consequently, there are less than 50 surgeons in the world who have had an experience of performing more than 500 operations, the outcomes improve with more experience. Post-operative management in patients who have had PTE is not the same as treating other post-operative cardiac surgical patients and requires intense monitoring, specialized training and experience. Many of the complications of this operation require the patient to be treated with ECMO, though most people can put a patient on ECMO, managing these patients require a lot of experience. At Narayana Health we have a cumulative experience of over 1,000 ECMO runs. A multidisciplinary team is involved in the evaluation of each and every patient to decide on the best way of treatment, which is known to improve the outcomes. The unpredictability of financial burden to the patient in case of complications or need for ECMO (which can far exceed the original estimate of operation cost) is offered as part of the operative package assuring predictability of expenses related to the operation. An expert centre for this disease, by definition, needs to have a volume of over 50 operations annually and be able to offer all the therapeutic options for these patients.
At present, no other hospital in the subcontinent meets the volume criteria for being an expert centre.

Experience of
over 1000 Pulmonary Thrombo
Endarterectomies (PTE)
One of the first centres in India to perform Pulmonary Endarterectomies - 23 years ago


Internationally-trained team
of cardiac specialists
State-of-the-art
infrastructure

Experience of
over 1000 Pulmonary Thrombo
Endarterectomies (PTE)
Internationally trained team
of cardiac specialists
One of the first centers in India to perform Pulmonary Endarterectomies over 23 years ago
State-of-the-art
infrastructure
Dr. Devi Prasad Shetty
MS. FRCS ( England)
Founder, Chairman and
Senior Consultant Cardiac Surgeon

Dr. Julius Punnen
MS, M.Ch (CTVS), FIACS
Senior Consultant
Cardiac Surgeon

Dr. Varun Shetty
DNB (CTS), FRCA (CTS)
Consultant
Cardiac Surgeon

Dr. Bagirath Raghuraman
MD, DNB, DM (Cardio), FICC, FSCAI
Senior Consultant
Interventional & Transplant Cardiologist

Dr. Basha J Khan
MD, MRCP, IDCCM, Fellowship (Toronto)
Senior Consultant
Pulmonology

Dr. George Cherian
MD, DM, Teaching Fellowship
Professor
Cardiac Surgeon

Dr. Karthik G A
MDRD
Senior Consultant
Radiologist

Dr. B.V. Murali Mohan
MD, MRCP (UK), SCE (Resp Med) UK, FRCP (UK)
Senior Consultant
Physician & Pulmonologist

Dr. Tanuj Gupta
DMRD, DNB
Consultant
Radiology

Dr. (Major) Vimal Raj
MBBS, FRCR, CCT (UK), PGDMLS, EDM
Consultant Cardiac and
Chest Radiologist

Dr. Ranganatha R
DTCD, DNB
Consultant
Pulmonologist
Opt for a right opinion from our experts to get a detailed re-evaluation, alongside a variety of alternative treatment options.

Resarch

In The News

Blog