Causes | Symptoms | Treatment
What is an aortic aneurysm?
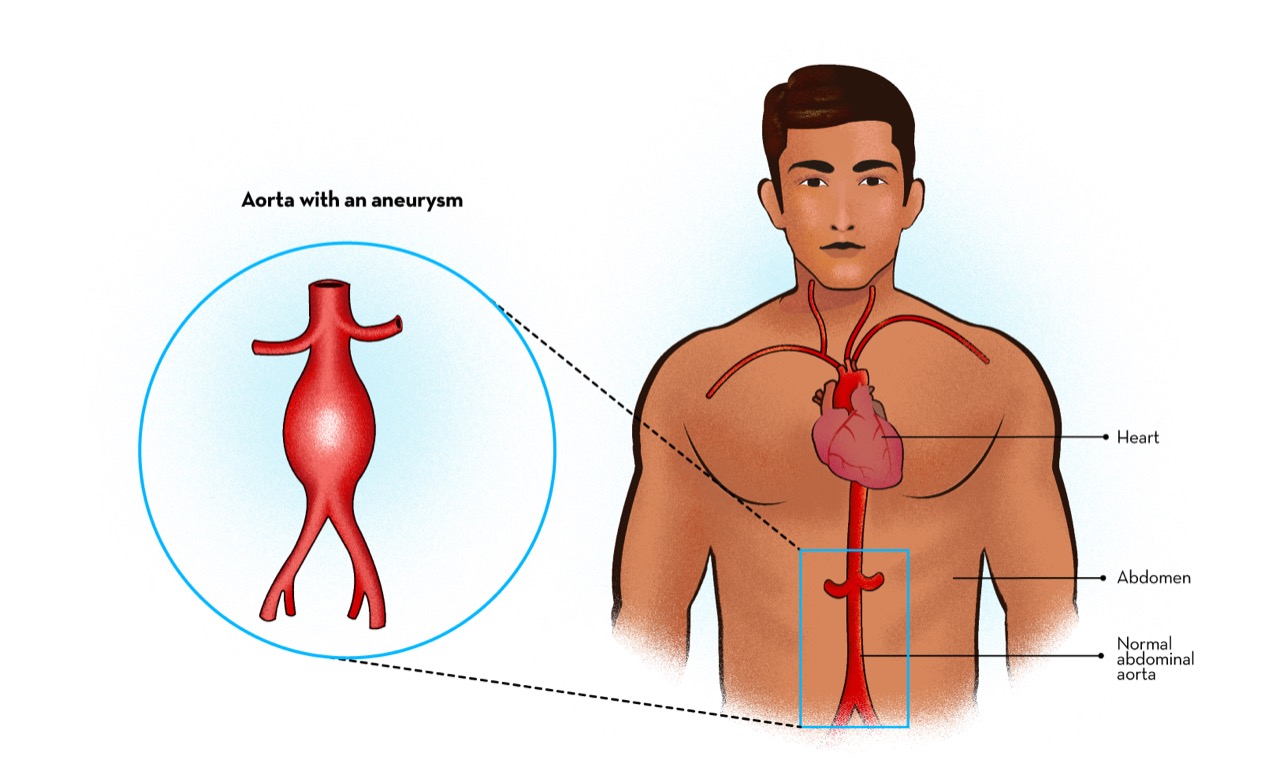
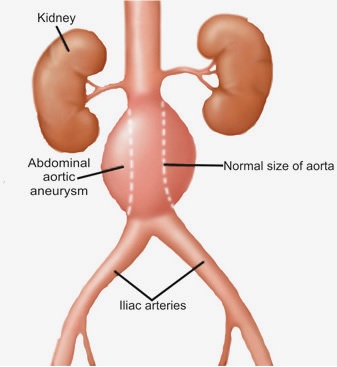
When the aneurysm occurs in the abdominal part of the aorta it is called abdominal aortic aneurysm. Abdominal aorta is the most common site for aortic aneurysm.
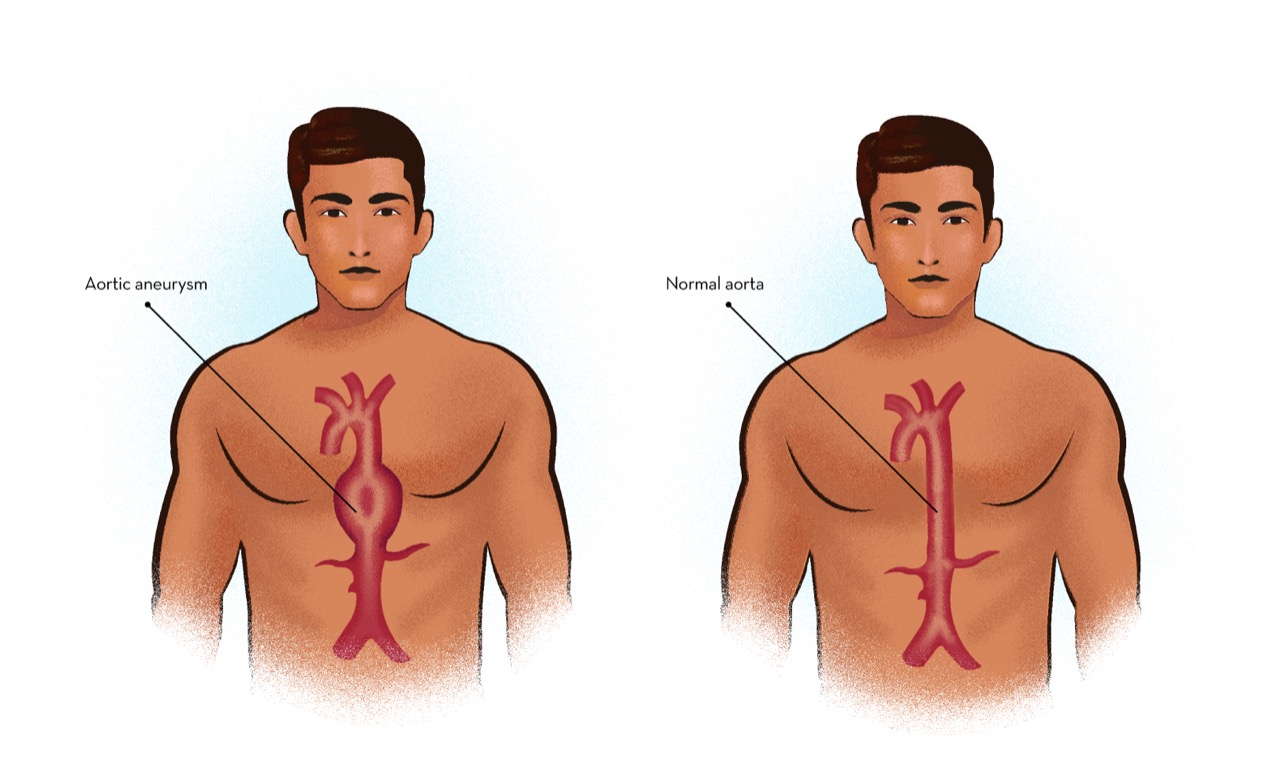
When the aneurysm occurs in the thoracic part of the aorta, it is called thoracic aortic aneurysm.
When the aneurysm occurs in both thoracic and abdominal part of the aorta, it is called Thoraco abdominal aortic aneurysm.
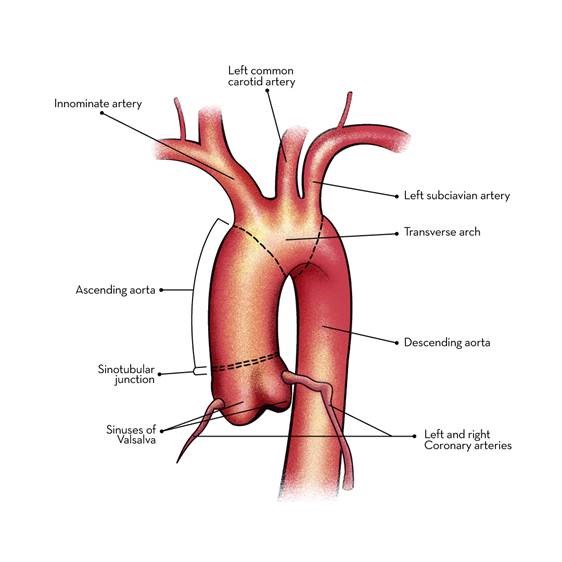
Aorta has three layers like a sandwich. The inner layer is called intima which is covered by media; which is covered by adventitia.
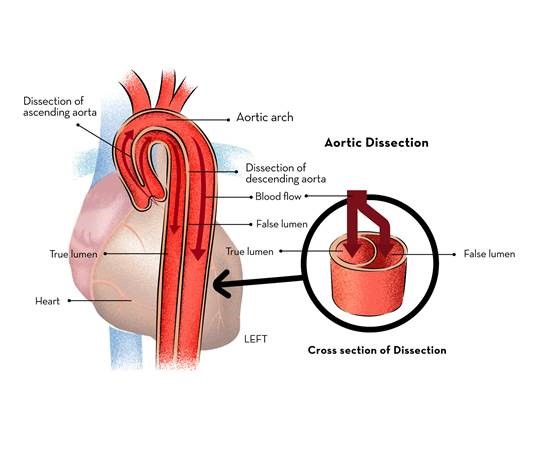
Aortic dissection or Dissecting Aneurysm of Aorta occurs when the inner layer of the aorta called intima develops a tear and blood under high-pressure separates the inner from outer layer of the media to produce a false lumen causing weakness and subsequent dilatation called aortic dissection or dissecting aneurysm of aorta.
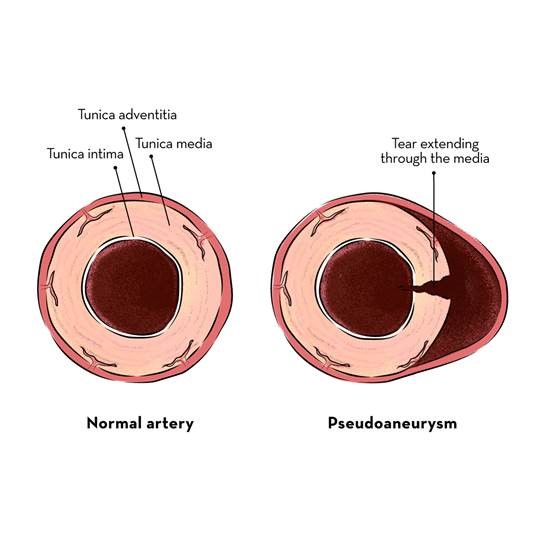
False aneurysm of aorta is a collection of blood surrounded by connective tissue outside the aortic wall. It happens due to small tear or small rupture of the aortic wall.
Incidence of aortic aneurysm for men is 16/100,000 population, slightly less in women.
Aortic aneurysms are commonly located in the abdominal aorta followed by thoracic aorta.
Causes of aortic aneurysms
Abdominal pain or pulsating abdominal lump from enlarging abdominal aortic aneurysm
Diagnosis of thoracic aortic aneuyrsm
In the initial stages, thoracic aneurysms grow slowly at about 0.1 cm per year. As the size increases, it grows faster.
Surgery is generally indicated for aneurysms larger than 5.5 cm in diameter. However, in Marfan syndrome surgery is indicated even when the aneurysm is smaller.
30-day mortality following thoracic aneurysm surgery is approximately 2.9%.
Survival following ascending aorta replacement, usually in combination with aortic valve replacement, is about 70% at 5 years and 50% to 60% at 10 years. Survival may be lower for patients who require urgent or emergency operation. Five year survival rate in operations on the aortic arch is about 80% for repair of the descending thoracic aorta, the five year survival rate is 71% in repair of thoracoabdominal aorta, the five year survival rate has been reported as 71%.
Success rates of elective operations on the ascending aorta is 97%, on the descending aorta is 97.1% and for thoracoabdominal aortic operations is 88.1%.
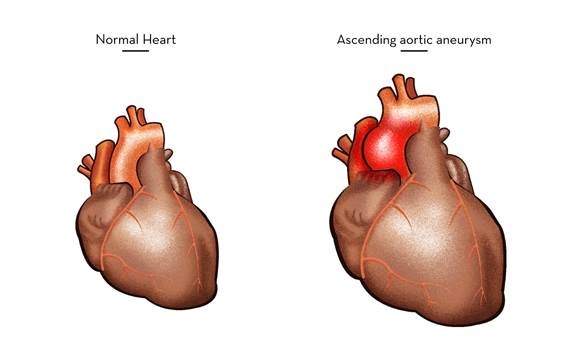
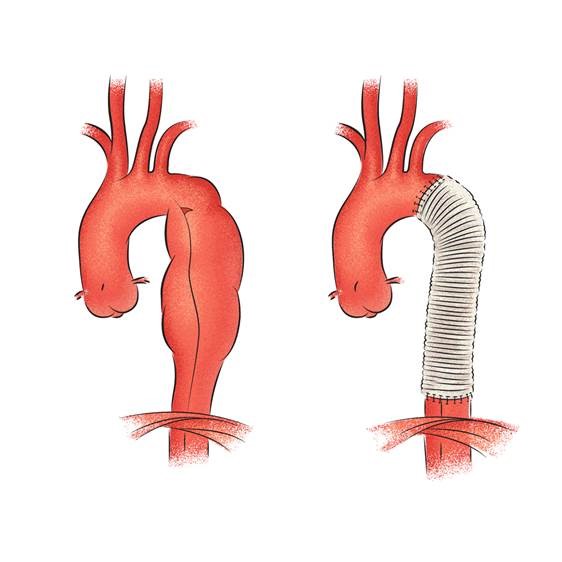
Causes of aneurysm of ascending aorta
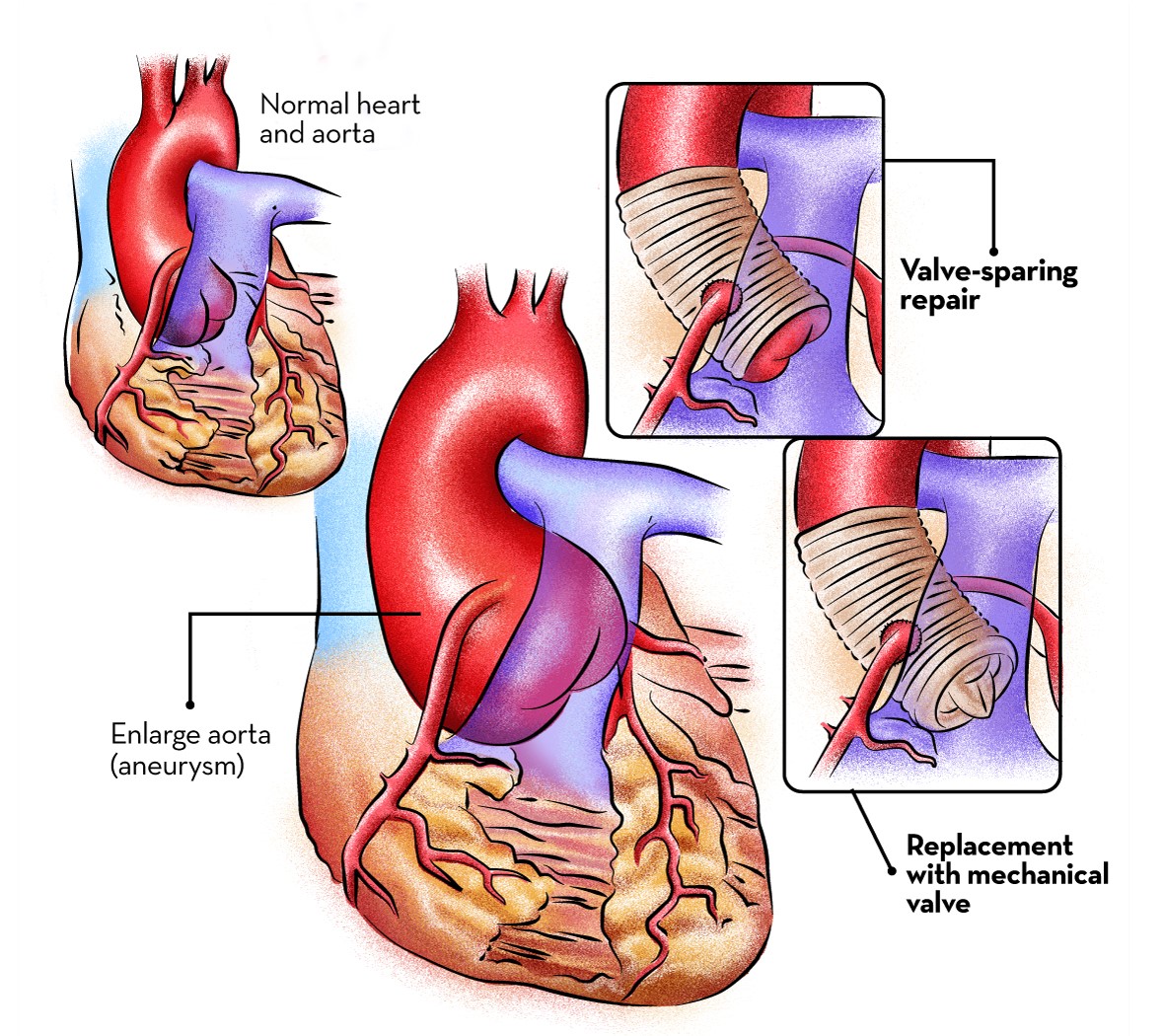
In David procedure, the patient’s own aortic valve is repaired and re-implanted inside a Dacron tube.
By preserving the patient’s own aortic valve, lifelong anticoagulation is not required
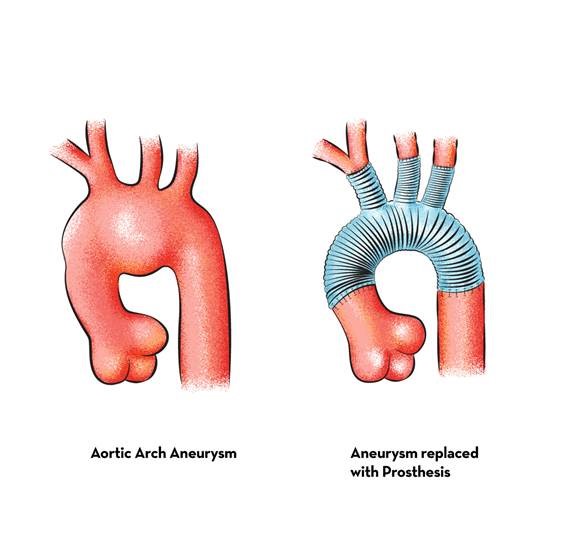
Replacement of aortic arch with the re-implantation of neck arteries
Causes of Descending thoracic aneurysm
Thoracic aneurysm is a very serious medical condition. If left untreated past the size of 5.5 cm in diameter can lead to sudden rupture or tear causing massive internal bleeding and sudden death.
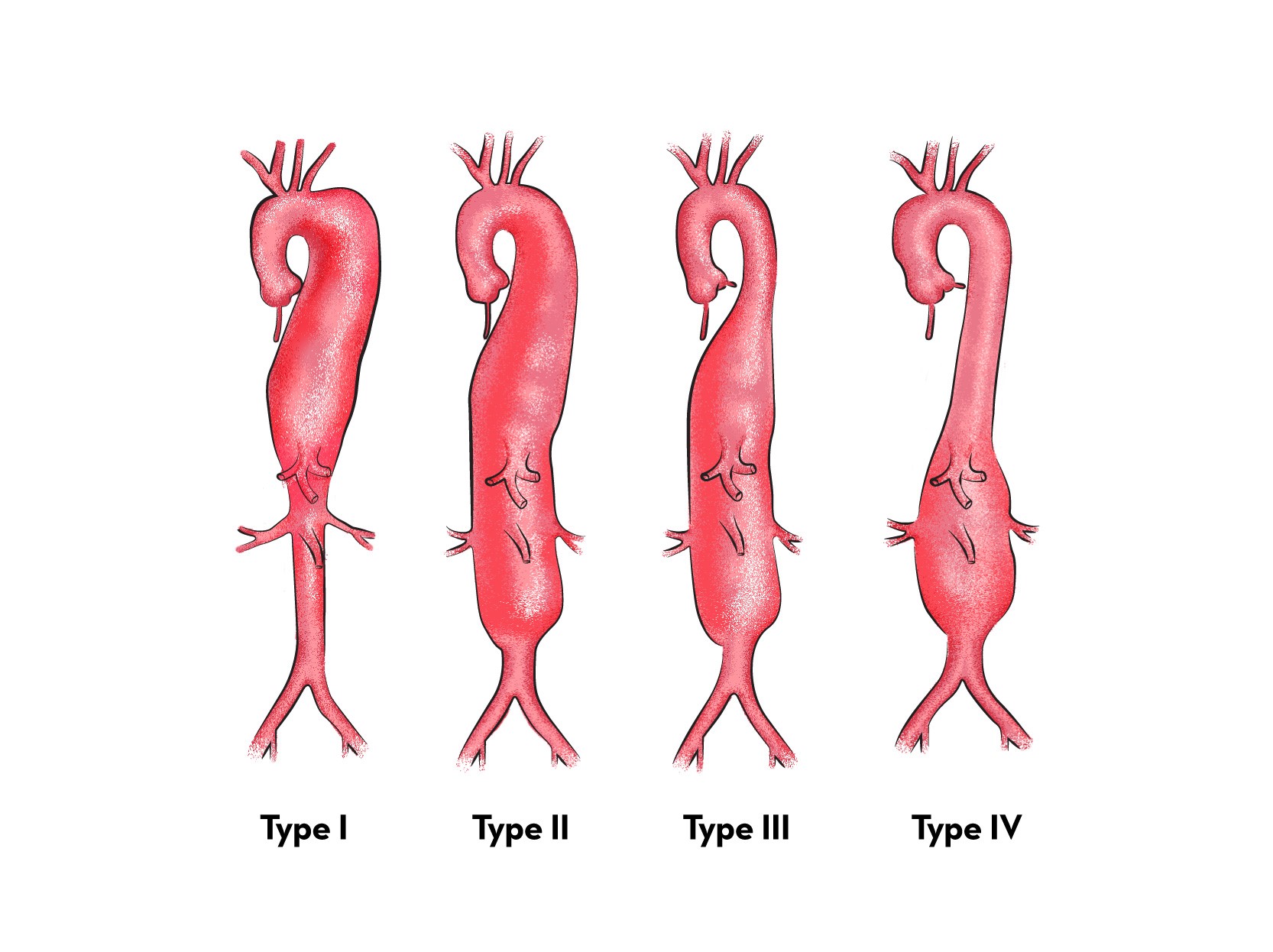
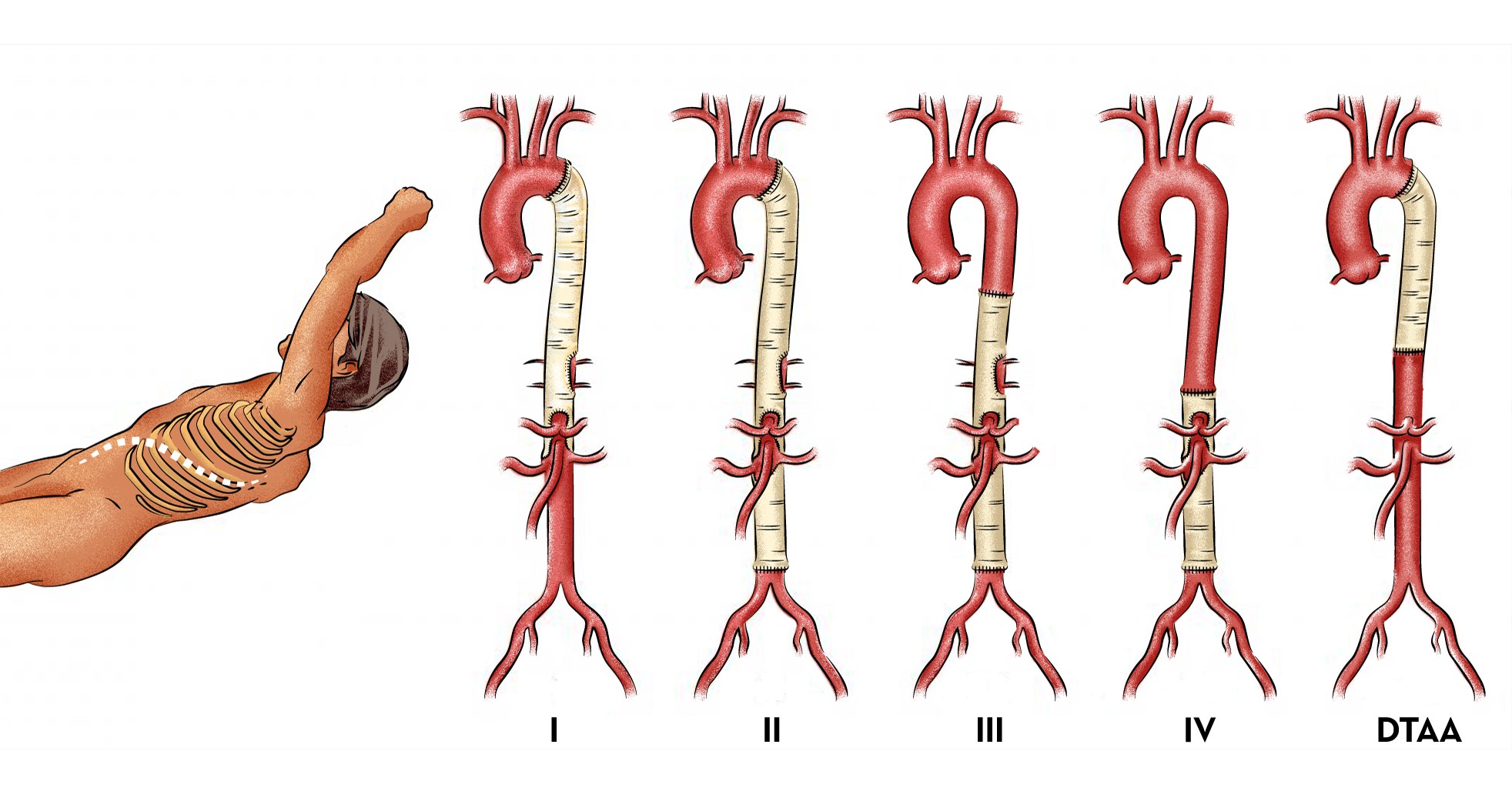
What is thoracoabdominal aortic aneurysm?
Thoraco abdominal aortic aneurysms are one of the most complex aneurysms to operate on. Open repair of thoracoabdominal aneurysm is one of the most extensive operations performed on the human body
What is abdominal aortic aneurysm?
Within the first few weeks surgical incision site pain gradually settles down. How ever, it will take at least 2 to 3 months time for the patients to get back to work.
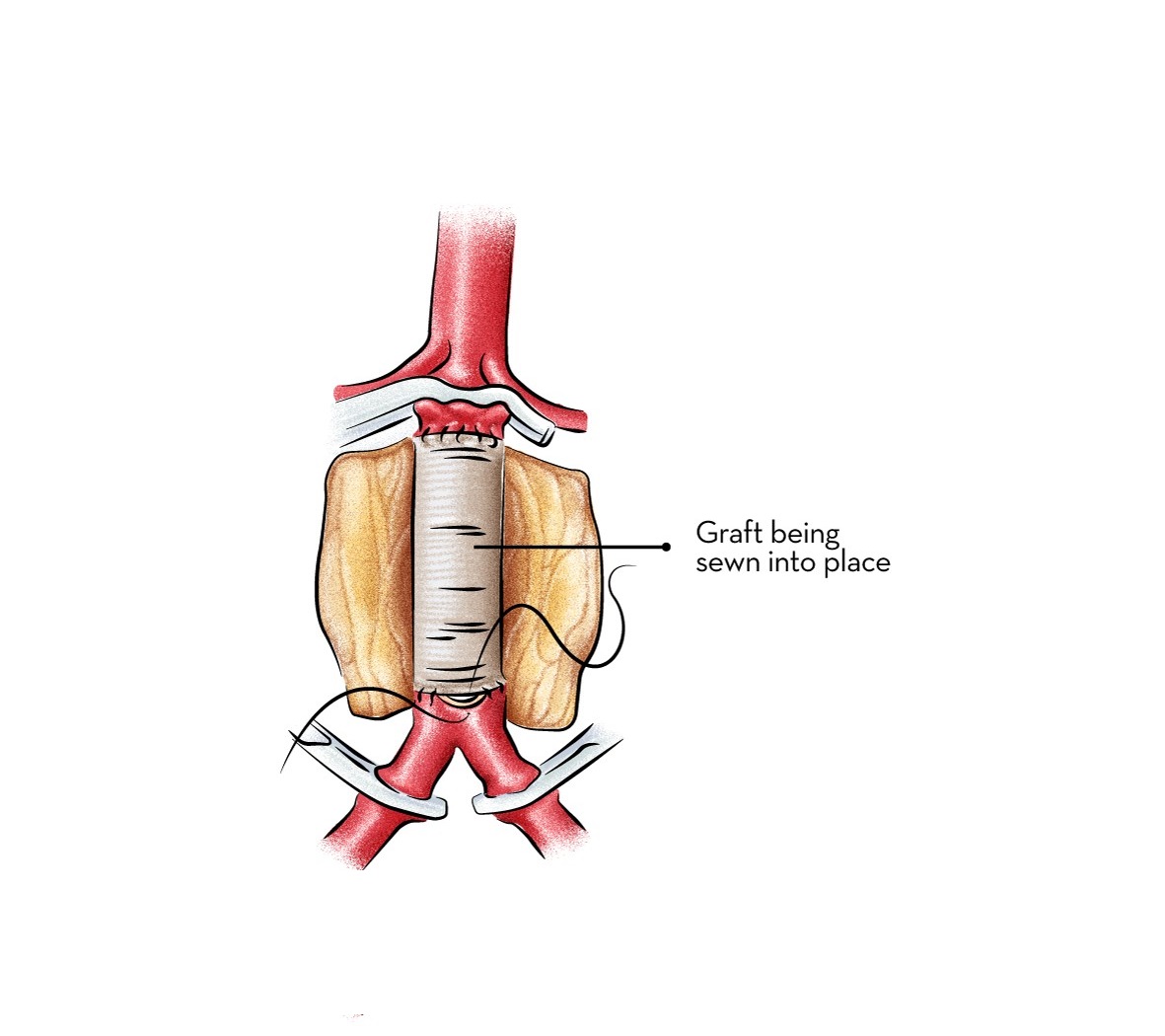
After successful procedure, problems of the graft is much lower with open surgery than endovascular surgery. Patients of open surgery need less scans and follow-up
What is endovascular surgery?
How is the recovery after Stent graft?
Standard recovery after stent graft is remarkably straightforward. Patients who have undergone stent graft typically spend one or two nights in the hospital to be monitored. Patients are advised to slowly return to normal activity. There are no specific activity restrictions after stent graft. Endovascular grafting procedures have very good outcomes. Patient needs follow-up visits for the stent graft, but most patients live a normal life after the procedure. In general, patients with aneurysms should follow a healthy lifestyle that includes a healthy diet and regular exercise.
As long as there are no infections and the stent graft doesn't move, they are known to last for a lifetime. Problems arise when the graft moves or the “seal” is lost (rarely) and the aneurysm sac starts to grow again. This is why, monitoring of stent grafts with CT angiograms or ultrasounds is very important. These rare cases can again be treated with stent grafting.
Up to 80 percent of aortic aneurysms are caused by "hardening of the arteries" (atherosclerosis). Atherosclerosis can develop when cholesterol and fat build up inside the arteries. High blood pressure (hypertension), cigarette smoking, family history and age also contribute to atherosclerosis. Atherosclerosis accelerates the breakdown of collagen and elastin, two proteins that provide strength, structure and elasticity to the wall of the aorta. Over time, this causes the walls of the aorta to weaken and become damaged. Elevated blood pressure through the aorta can then cause the aortic wall to expand and bulge.
Aortic aneurysms often have no symptoms at first; in fact, many are first discovered during an examination for another condition. If the aneurysm is pressing against nearby tissues, patients may notice a deep, steady pain in the back, abdomen or groin. Abdominal aortic aneurysms may also cause a pulsing sensation in the abdomen.In most cases, an unruptured abdominal aortic aneurysm (AAA) will cause no symptoms, unless it becomes particularly large.
If the aneurysm continues to expand, it can rupture. The layers of the aortic wall can also separate (aortic dissection). This produces severe, tearing pain in the chest, back or abdomen. The potential for rupture is the most serious risk associated with an aortic aneurysm. A ruptured aortic aneurysm can cause life-threatening internal bleeding and/or a stroke.
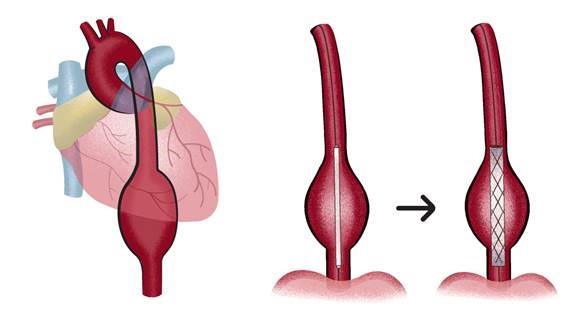
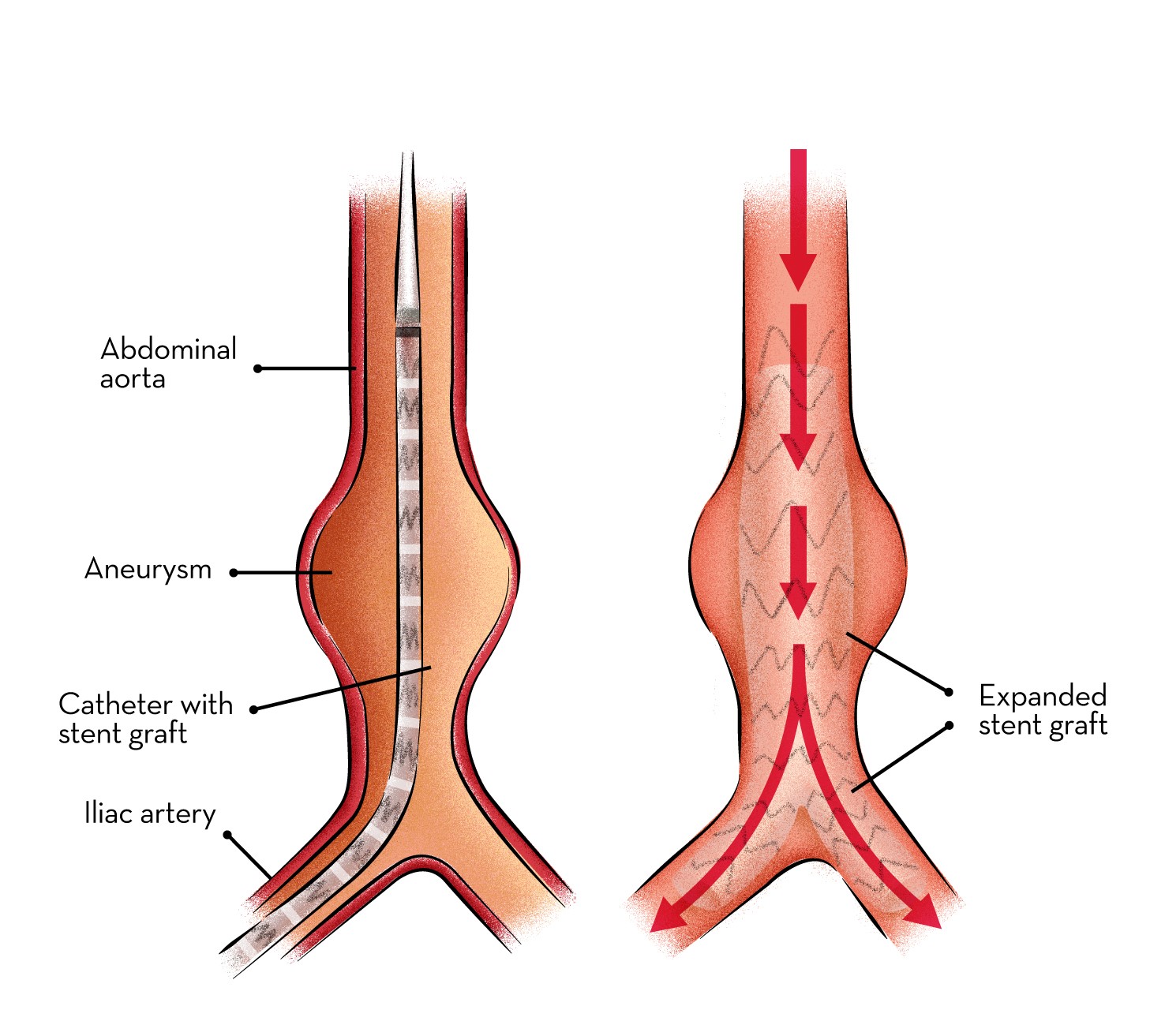
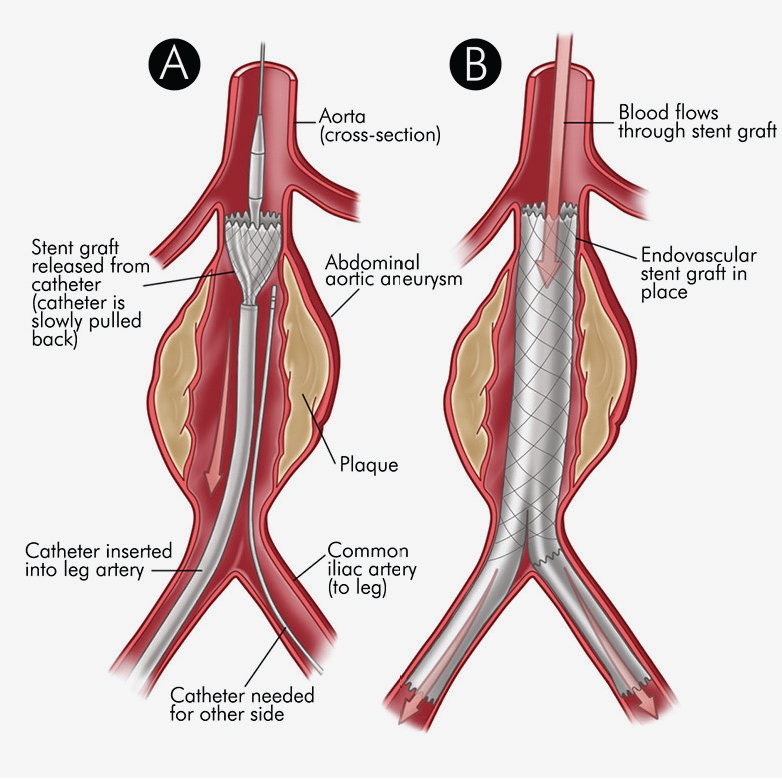
Stent grafts are used in transcatheter endovascular aortic repair (EVAR) procedures to seal aortic aneurysms. The grafts usually consist of a self-expanding stent frame that is covered with material to seal the vessel walls and prevent blood leaks feeding the aneurysm.The stent graft is a tube made of a thin metal mesh (the stent), covered with a thin polyester fabric (the graft). The tube is collapsed so it is narrow and can fit through your blood vessel. When the stent graft reaches the aorta, it is opened up and fastened in place.
The procedure is carried out in a sterile environment under fluoroscopic (X-ray) guidance. The procedure can be performed under general, regional (spinal or epidural) or even local anaesthesia. After accessing the patient's femoral arteries (leg arteries), vascular sheaths are introduced into them, through which guide wires (small calibre wires), catheters (plastic tubes) and the endograft (stent graft) are passed. Diagnostic angiography (images of disease segment) of the aorta helps to determine the location of the patient's arteries, so the stent graft can be deployed without blocking these. The “main body” of the endograft is placed first, followed by the “limbs” which join the main body and extend to the iliac arteries, effectively protecting the aneurysm sac from blood pressure. The endo graft acts as an artificial lumen for blood to flow through, protecting the surrounding aneurysm sac. This reduces the pressure in the aneurysm, which itself will usually thrombose and shrink in size over time. The procedure itself generally takes 2 to 3 hours. Patient will stay in the hospital for 1 to 2 days. Full recovery will take about a month
How does the heart work?
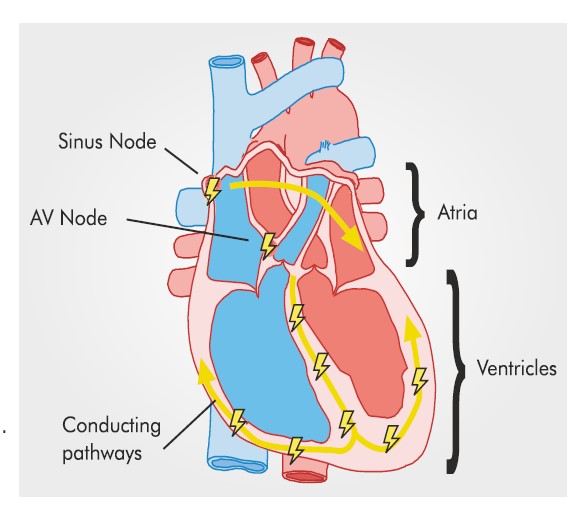
The heart pumps blood that circulates throughout the body.
An integrated electrical system controls the pumping of blood and its circulation.
The pumping of heart at regular intervals is called heartbeat.
The number of times a normal heart beats in a minute is called heart rate.
The normal adult heart beats 60-100 times in a minute.
Trained athletes and elderly individuals tend to have a heart rate lower than 60 beats/minute.
For children, the normal heart rate is 100-150 beats/minute.
When the heart rate of an individual is above or below the normal heart rate, it is considered to be a heart rhythm disorder.
This condition is also referred to as ‘arrhythmia’.
A slow heart beat is referred to as ‘bradycardia’.
An increased heart rate is called ‘tachycardia’.
A drop beat is a transient pause in the heart rhythm.
An extra beat is called ‘Ectopic beat’.
In a lot of instances, this is not a serious cause of concern but its frequent occurrence can be an indicator of arrhythmia.
Arrhythmia may occur to anyone from new born children to adults.
It becomes more common with advancing age.
It may be associated with structurally normal heart as well as with other disorders of heart like valve diseases.
Arrhythmia displays a wide range of symptoms that can be detected in both adults and children.
In adults, the symptoms include skipped heartbeats palpitations, rapid or irregular heartbeat and difficulty in breathing.
Children may experience constant weakness, shortness of breath, lightheadedness and difficulty in eating/feeding in addition to skipped, rapid or irregular heartbeats.
In extreme cases patient may lose consciousness.
Arrhythmia impairs the electrical system of the heart and results in improper blood supply to the body.
This can lead to a heart failure, loss of consciousness, and in some cases sudden cardiac death.
It can also create blood clots that may move to the brain to cause a stroke.
An electrocardiogram (ECG) and echocardiogram are used by the doctors to detect arrhythmia.
Tests such as Holter or external loop recorders are available to monitor the heart rate over a long term.
An advanced option for detecting abnormal heart rhythm is electrophysiology studies.
Electrophysiology is a branch of cardiology that studies the electrical makeup of the heart it's disorders, that is arrhythmia.
It employs a minimally invasive procedure where an electrically sensitive cardiac catheter* is placed in the heart and the electrical conduction is studied.
*A cardiac catheter is a long, flexible, thin tube that is inserted into a large blood vessel (in the arm, groin or neck region) that leads to the heart.
An Electrophysiologist is a cardiologist who specializes in the electrical system of the heart and heart rhythm disorders.
Radiofrequency Ablation (RFA) is a procedure performed to treat a rapid heartbeat.
A physician guides a catheter with an electrode at its tip to the damaged or abnormal area of the heart muscle.
Then mild, painless radiofrequency waves (similar to microwave heat) are administered to the heart muscle cells in a very small area (about 1/5 of an inch or the size of a pencil eraser).This stops them from conducting the extra impulses that caused the rapid heartbeats.
In cases of slow heart beat or Bradycardia, a device called Pacemaker is implanted in body (by minimally invasive technique), which maintains appropriate heart rate by giving electrical impulse when needed.
Cardiac Resynchronisation Therapy is another device like Pacemaker, which can be implanted to improve the pumping capacity (EF) of heart in selected cases.
In patients with risk of sudden cardiac death, an Implantable Cardiac Defibrillator (ICD) could be lifesaving. It is a device that is implanted like a pacemaker and has the ability to diagnose and deliver life saving shock appropriately in selected individuals with risk of sudden cardiac death.
Arrhythmia can greatly affect the quality of life of the patient. EPS/RFA have been successful in effectively treating arrhythmia.
It is a more convenient alternative to a medication regime. Medicines will need to be taken daily and life long with potential side effects. They may also need to be changed frequently.
Almost all electrical disorders of the heart can be treated with advanced 3 Dimensional EPS/RFA system and device therapy today.
EPS/RFA have displayed an acute procedural success of 90-95% for most of the arrhythmias.
The recurrence rate is between 5-10% for most of the arrhythmias treated with EPS/RFA.
All procedures involve some small risks. The risk associated with most electrophysiology procedures is less than 1%.
The risk is higher in sick patients and it is advised to consult us early.
Major life threatening complications are very rare, and can be managed with timely treatment.
The typical duration of stay is 24-48 hours in the hospital.
Ejection fraction is the measurement of how much blood is being pumped out of the heart. The ejection fraction of a healthy individual is between 55% and 70%.
The left ventricle is the major pumping chamber of the heart. If the Left Ventricular Ejection Fraction (LVEF) drops below 35%, the patient may be at risk of developing an arrhythmia.
This drop may even lead to sudden cardiac death which can be prevented with the help of an Implantable Cardioverter Debrillator (ICD) to constantly monitor the heart. During an arrhythmia, the ICD gives an electric shock to the heart and brings it back to the normal rhythm.
Syncope is the sudden loss of consciousness. If the reason behind the fainting episode is known to be harmless (e.g. standing in the heat), it is not a cause for concern.
When the reason for the syncope is unknown, it may be caused by arrhythmia. Hence, it is recommended to consult a cardiologist in such a case. They may perform an electrocardiogram (ECG) to assess the cause.
We, at Narayana Health, take pride in our excellent electrophysiology division with distinguished experts with subspecialty expertise. Our world-renowned electrophysiologists specialize in both pediatric electrophysiology and adult electrophysiology.
Treatment of aortic aneurysm is one of the most complex procedures done on the human body, particularly surgical treatment of thoracoabdominal aneurysm. A good outcome depends on an array of factors including expert doctors across several disciplines and a slew of facilities. When it comes to doctors, the procedure needs to have cardiologists, cardiovascular surgeons, interventional cardiologists, radiologists, anaesthesiologists, perfusionists, physiotherapists and dietitians. The facilities required include a well-equipped intensive care unit with specialist physicians, a blood bank capable of offering various specialised blood products often at short notice and availability of all these personnel and services round the clock. Many centres shy away from doing these complex operations due to lack of adequate infrastructure and/ or trained human resource.
At Narayana Health, these operations are done in large numbers with excellent outcomes by people who have had specialised training and experience in performing this operation. The multidisciplinary approach helps to tailor the best treatment for any given patient making the overall treatment safer and more effective. Narayana Health group is one of the few hospitals to have a hybrid operation theatre that includes cardiac catheterisation labs to perform procedures that need a combination of open and interventional procedures.
Treatment of aortic aneurysm is one of the most complex procedures done on the human body, particularly surgical treatment of thoracoabdominal aneurysm. A good outcome depends on an array of factors including expert doctors across several disciplines and a slew of facilities. When it comes to doctors, the procedure needs to have cardiologists, cardiovascular surgeons, interventional cardiologists, radiologists, anaesthesiologists, perfusionists, physiotherapists and dietitians. The facilities required include a well-equipped intensive care unit with specialist physicians, a blood bank capable of offering various specialised blood products often at short notice and availability of all these personnel and services round the clock. Many centres shy away from doing these complex operations due to lack of adequate infrastructure and/ or trained human resource.
At Narayana Health, these operations are done in large numbers with excellent outcomes by people who have had specialised training and experience in performing this operation. The multidisciplinary approach helps to tailor the best treatment for any given patient making the overall treatment safer and more effective. Narayana Health group is one of the few hospitals to have a hybrid operation theatre that includes cardiac catheterisation labs to perform procedures that need a combination of open and interventional procedures.

Internationally trained team
of cardiac specialists
State-of-the-art
infrastructure

Internationally trained team
of cardiac specialists
State-of-the-art
infrastructure
Dr. Devi Prasad Shetty
MS. FRCS ( England)
Founder, Chairman and
Senior Consultant Cardiac Surgeon

Dr. Julius Punnen
MS, M.Ch (CTVS), FIACS
Senior Consultant
Cardiac Surgeon

Dr. Varun Shetty
DNB (CTS), FRCS (CTS)
Consultant
Cardiac Surgeon
Dr. Robbie George
MS, PDCC, DNB, FRCS
Senior Consultant
Vascular Surgeon

Dr. Sanjay Mehrotra
MBBS,MD,DM
Senior Consultant
Cardiologist

Dr. (Major) Vimal Raj
MBBS, FRCR, CCT (UK), PGDMLS, EDM
Consultant Cardiac and
Chest Radiologist

Dr. Karthik G A
MDRD
Senior Consultant
Radiologist
Opt for a right opinion from our experts to get a detailed re-evaluation, alongside a variety of
alternative
treatment options.

Resarch

In The News

Blog